
Given his experience of the Ombudsman you would expect James Titcombe to know better, but when he posted Rob Behrens’s blog on his Patient Safety Watch page (HSJ) he described it as ‘insightful’. For real insight we need to look at what has been left out.
The struggle continues, by Rob Behrens
The omens were not good in 2017 when I was appointed as parliamentary and health service ombudsman.
In addition to a 24 per cent budget cut prompting an exodus to Manchester, there was published ministerial displeasure at the insensitive way in which PHSO dealt with families who had lost children in the health service. In addition, staff morale was very low.
A key omen is the customer satisfaction scores which actually show a higher score during the time of his predecessor Dame Julie Mellor than he managed to achieve in the following two years. Unsurprisingly, they stopped gathering the data in this format after 2018/19.

What transpired from a long consultation to create consensus about the way forward and the values associated with that path was a strategic agenda rooted in professional development for all staff, and a commitment to the principle of transparency with the ambition (now achieved) of publishing casework outcomes.
There was no consensus when it came to communications with service users who had joined PHSOtheFACTS. Following a meeting with Rob Behrens 10.10.2017 he closed down opportunities for further contact with the group on 22.11.2017.
The ‘mechanisms outlined’ were to attend the annual open meeting and listen to the radio ombudsman podcast which were hardly interactive forums.
There was also an engagement with service providers on the fundamentals of effective complaints handling on the frontline of service delivery.
The significant achievements in professional development included a portfolio of professional training to promote better investigations and aligned to patient safety issues, the requirement that senior caseworkers be accredited to demonstrate their competence, and the creation of an Ombudsman Academy (the first in Europe) to oversee the development of a generation of new case handlers as the office expanded and most casework staff moved to Manchester.
The biggest challenge here was to address the significance of patient safety as a central strand in ombudsman work. I commissioned Sir Liam Donaldson, formerly the chief medical officer and not known for his reticence, to review independently the clinical advice function of the ombudsman service.
Rob Behrens omits the fact that the clinical review undertaken by Sir Liam Donaldson was commissioned following a successful judicial review against the Ombudsman in February 2018 which was critical of the way in which PHSO handled external clinical advice. Sir Liam discusses this court judgement on page 10 of his report.
Any criticism especially by an external entity that is itself perceived as impartial is potentially very damaging to the PHSO’s reputation and public image. This is especially so if a court is making the criticism. A recent example is a judgement of the Court of Appeal (Civil Division) on the case of two doctors, Miller and Howarth, and The Health Service Commissioner for England (one of the Ombudsman’s titles in legislation and used to refer to him by the Court) (25). The doctors lodged an appeal against The Health Service Commissioner’s decision to uphold a complaint against them. The Court of Appeal found for the doctors and criticised various aspects of the handling of the complaint by The Health Service Commissioner’s staff, particularly the commissioning, use, communication and standard employed in the clinical advice to assess, investigate and adjudicate the complaint. The case dated from 2012, where the PHSO position had originally been upheld in the High Court and many of the criticisms related to ways of working that were out-dated by the point of the judgement. This is why the PHSO did not appeal and decided instead to address the fundamental outstanding issue in relation to the Clinical Standard.
p.10 https://www.ombudsman.org.uk/sites/default/files/PHSO_Clinical_Advice_Review_Report_of_Independent_Adviser.pdf
Rob Behrens is particularly proud of his work in training and accrediting ombudsman staff, but Sir Liam’s report reveals that this internal process was simply validating unsound practice.
On reading the judgement, it is a perfect example where the internal world and the external world see things differently. Those handling the complaint believed themselves to be following the normal rules, customs and practices. Yet, the account of the Appeal Court Justices on the handling of the complaint brings an entirely reasonable expectation from the external world that decisions and actions should be appropriate and fair. The PHSO’s team in this case believed that their work was procedurally sound. Impartial scrutiny found that they were not.
p10 https://www.ombudsman.org.uk/sites/default/files/PHSO_Clinical_Advice_Review_Report_of_Independent_Adviser.pdf
Was it necessary for Rob Behrens to create the ‘Ombudsman Academy’ because it was impossible to gain external validation from an existing academic organisation? It would appear from Sir Liam’s report that PHSO case handler training is rigid, top-down and not fit for purpose.
The handling of complaints by the PHSO service is very procedurally driven. In part, this is because of legislation governing the PHSO role in NHS complaints, in part because of internal procedures, both written and unwritten. Both are underpinned and reinforced by the induction, training and supervision of the organisation’s staff. Generally, close adherence to these procedures is important and a good thing but not when they do not serve a necessary wider purpose (e.g. of safeguarding future patients from harm) or when they discourage thinking and common sense reasoning (e.g. not taking up a serious concern about care because it is not one of the strands of the complaint) or when they confuse and upset too many complainants. Some staff are very protective of the current procedures and seem to hold the belief that, because of the statutory role of the PHSO, little can be changed.
p9 https://www.ombudsman.org.uk/sites/default/files/PHSO_Clinical_Advice_Review_Report_of_Independent_Adviser.pdf
Rob Behrens omits all this information in his blog and focusses attention only on the following points.
In his [Sir Liam Donaldson] view, external clinical advisers were too peripheral to the investigation process and should test and challenge the views of case handlers without departing from their advisory role. He also thought that the clinical advice team required decisive professional leadership from an inhouse clinician to align it more effectively to the Ombudsman’s patient safety agenda. In terms of developing trust, he wanted complainants to be able to see the clinical advice that was provided.
All but the last of these recommendations have been implemented.
The legal judgement made it clear that the subject of the complaint should be given the opportunity to review the clinical advice received by the Ombudsman before a decision is made.
“…for complaints adjudicators who rely on expert evidence to reach findings of fault or service failure then there should be early disclosure of those expert reports alongside so that the subject of the complaint has an opportunity to see and fully respond to the case against them.”
https://www.bevanbrittan.com/insights/articles/2018/court-of-appeal-overturns-health-ombudsmans-decision-on-gp-medical-care/
As Sir Liam’s recommendation to share clinical advice with the complainant has not been implemented, they will be unable to comment until after the decision is made. This is a clear disadvantage to the complainant.
The result is the national ombudsman service having the capacity to make more rigorous decisions about individual cases involving patient safety. We have supplemented Sir Liam’s work with the creation of both a working group of ombudsman and deputy ombudsman leaders to have close oversight of complex cases and a small expert advisory panel to give supplementary advice.
Further, we now have the organisational coherence to make interventions in systemic patient safety issues. This has led (for example) to our regular engagement with health service regulators, and given us the confidence to trigger publicly the Emerging Concerns Protocol over long failures at University Hospitals Birmingham Trust to place patient safety above its own reputation.
The suggestion here is that prior to Sir Liam’s report PHSO lacked the organisational coherence to make interventions in systemic patient safety issues which is a sorry admission of failure for all those who have suffered as a consequence. But in essence has anything really changed? From Rob Behrens interview on BBC Newsnight in relation to the failures at University Hospitals Birmingham Trust (UHB) we learn that the Ombudsman was excluded from a key review. Perhaps NHS England continue to doubt the organisational coherence of PHSO.
Mr Behrens wrote his organisation had been excluded from the NHS England-led review into UHB, expressing his disappointment that evidence held by the ombudsman would not be considered.
“PHSO’s (Parliamentary Health Service Ombudsman) exclusion from the review process leaves me concerned about the completeness and transparency of the reviews,”
We have also used ombudsman clinical expertise to point to failures in imaging services in the NHS and to detail in accessible fashion of the adverse lived experiences of women in childbirth and under perinatal care and we are poised to make an evidence-based contribution to the national covid inquiry, where we will draw attention to malfunctioning of Do Not Resuscitate procedures remote access to care and poor communication with patients.
Is PHSO then the exemplary ombudsman service it set out to become in its 2018 corporate strategy? Five years down the line, and in the opinion of international ombudsman peer review, the answer is “not yet” but that we are well on the way. The latest peer review by counterparts in Greece, Israel, and the Housing Ombudsman Service in England pointed to significant success in reviving staff morale and engagement.
But, they returned to the point about the sorry refusal of ministers to provide time for legislative reform to develop our mandate in a way which would contribute substantially to addressing continuing issues of patient safety.
Two, much needed, reforms stand out. The first is the creation of a single public service Ombudsman for England uniting at commencement PHSO with the Local Government and Social Care Ombudsman. This integration would join up the oversight and investigation of health and social care complaints under one roof. When established it would make much clearer where to go to complain.
Equally important and routine across Europe are the powers of “Own Initiative” which give ombudsman offices the opportunity to investigate issues not directly complained about. By contrast, our own investigation into the deaths of young people in an Essex mental health facility was severely constrained by our inability to look at the substantial number of cases where the families of those who died had not complained.
A key case with regard to the Essex mental health facility was that presented by Melanie Leahy who lost her son Matthew while he was in the care of the trust. In the book ‘What’s the point of the Ombudsman?‘ Melanie Leahy gives the following description of the ombudsman investigation process.

No amount of ‘own initiative powers’ can make up for a biased investigation process.
In all these circumstances, the national ombudsman in the UK stands recrudescent and up for the fight, but impaired by government inaction on the legislative front. And it is impaired at a time when it is most needed. Public satisfaction with the NHS is at its lowest recorded level.
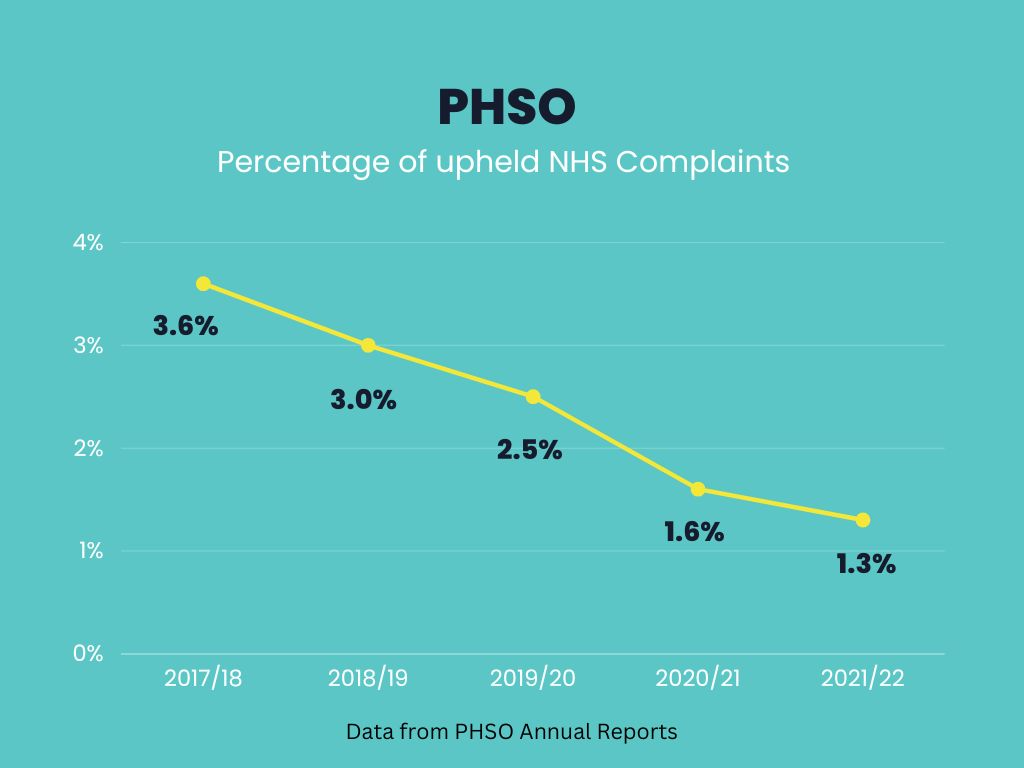
Equally, public confidence in the Ombudsman is impaired by its low investigation and uphold rate.
This is contextualised by a variable health service culture which, when patient safety is at stake, too often prefers turning on whistleblowers, to preserve organisational reputation. The challenge to the national Ombudsman is to continue to work independently, impartially and in evidence-based fashion to “speak truth and to power” through these turbulent times. The struggle continues.
I just can’t begin to unpick the empty rhetoric in this final paragraph except to say that according to the many 1 star reviews on Trustpilot PHSO is a total failure on all fronts.
Rob Behrens, parliamentary and health service ombudsman
Rob Behrens, master of spin.

Parliamentary question from Rachael Maskell:
UIN 187870, tabled on 5 June 2023
‘To ask the Secretary of State for Health and Social Care, whether he has taken recent steps to (a) review the level of satisfaction and (b) seek views on how better to resolve the disputes of patients using the complaints systems in the NHS.’
https://questions-statements.parliament.uk/written-questions/detail/2023-06-05/187870
PHSO is mentioned in the response. Not reassuring.
LikeLike
It doesn’t answer the question at all. Particularly on levels of satisfaction. Hope she asks a follow up.
LikeLike
You’ve said in this post the independent review said PHSO should share the clinical advice with the complainant before issuing a decision. However to support this, you quote a paragraph that says the advice should be shared with the “subject” of the complaint.
The “subject” isn’t the complainant.
LikeLike
Rob Behrens put the recommendation in his blog – Quote “In his [Sir Liam Donaldson] view, external clinical advisers were too peripheral to the investigation process and should test and challenge the views of case handlers without departing from their advisory role. He also thought that the clinical advice team required decisive professional leadership from an inhouse clinician to align it more effectively to the Ombudsman’s patient safety agenda. In terms of developing trust, he wanted complainants to be able to see the clinical advice that was provided.” RB also said that this last point had not been implemented. I then quoted from the legal judgement which said that clinical advice should be shared with the subject of the complaint following the upheld JR. Sir Liam was attempted to level the playing field by ensuring that both parties were provided with the clinical advice but unfortunately, Rob Behrens has not followed this advice, even though he is now legally responsible for sharing with the subject creating an unlevel playing field. Hope this clears up any confusion.
LikeLike
I have no doubt that the PHSO are monitoring and reading this blog and postings. However if they are then they may not be able to legally justify why they are doing so.
LikeLike
Who’d have thought that the PHSO under Behrens would be worse than under Mellor? James Titcombe was one the establishment slip through the net, now he’s part of the network people are up against in the fight for justice. You’re right Della, all political parties are in on this, and all our regulatory bodies are in the same sorry state, corrupt.
LikeLike
One must address where the real responsibility for this fiasco lies.
Who makes the legislation? – Politicians
Who appoints the Ombudsman? – Politicians
Who scrutinises the Ombudsman’s work? – Politicians.
It is seven years since Chris Skidmore MP heralded the draft bill outlining the “People’s Ombudsman’. That bill was flawed and fortunately failed to see the light of day due to lack of parliamentary time.
From what I have seen of the PACAC scrutiny sessions, the politicians are masters at ignoring the public submissions of evidence when it comes to interrogating the Ombudsman. Not surprising as they know that proper Ombudsman reform will only open the can of worms that exists within the NHS and Government Departments.
Bearing in mind that PACAC is a cross party committee, I am not convinced that things will improve with a change of government.
LikeLiked by 1 person
Me neither David. MPs of all colours are part of the problem
LikeLiked by 1 person
Great blog, nailing Behrens deceptive and misleading rhetoric. The omens were indeed not good when he was appointed Ombudsman in 2017. Under the previous Ombudsman the PHSO investigated 3,715 complaints in 2016-17. Under Behrens the PHSO investigated 612 complaints in 2021-22. An 83% decline in service to the public. The struggle does indeed continue, to get an Ombudsman service that is fit for purpose.
LikeLiked by 2 people
It appears from your reluctance to answer my last question that you, or the organisation you work for, are used by the PHSO
LikeLike
This much is true ‘Public satisfaction with the NHS is at its lowest recorded level.
This is contextualised by a variable health service culture which, when patient safety is at stake, too often prefers turning on whistleblowers, to preserve organisational reputation. The challenge to the national Ombudsman is to continue to work independently, impartially and in evidence-based fashion to “speak truth and to power” through these turbulent times. ‘ but but…I have little faith in PHSO given its record, evidence from patients, and the few exceptions which prove the rule
LikeLiked by 1 person
“Public satisfaction with the NHS is at its lowest recorded level. This is contextualised by a variable health service culture which, when patient safety is at stake, too often prefers turning on whistleblowers, to preserve organisational reputation.”
I can testify that the NHS puts self interests before patient safety and deception before candor. Derbyshire Healthcare NHS Foundation Trust is an expert in cover ups, aided by their friends at PHSO. In my case, the Trust’s CEO, Steve Trenchard, was friends with Mick Martin, PHSO’s MD, and they colluded to destroy the original report that upheld my complaint, based on independent clinical advice, into one that didn’t:
LikeLike
Given you purport to not be an employee of the PHSO then are you, or the organisation you work for, used by the PHSO ?
LikeLike
James Titcombe has chosen to ignore everyone else who has been failed. But I expect if he did offer support he would not be given a platform
LikeLiked by 1 person
Yes our James has been pulled inside the tent unfortunately.
LikeLiked by 2 people
Yes, he did me, when I approached him for advice. Ditto Julie Bailey. They forget they too were once reliant on help from others. Now they seem part of the establishment.
LikeLiked by 1 person
What is abhorrent about the PHSO is that any challenge of any kind to any of their decisions is responded to be any almost immediate smearing of the complainant by the PHSO by falsely suggesting that they have upset the PHSO caseworker and that they will no longer engage unless the complainant behaves themselves; in other words the complainant has already suffered and followed the MP referral procedure to the PHSO (it being significant that the MP had found the complaint to be valid and the complainant not to be the sort of person who goes around upsetting others or using inappropriate language) but then suffers even more at the hands of the PHSO many of whose staff are able and willing to lie to try and destroy a complainant who dares challenge them. If there caseworker/management staff were professionals such as solicitors or doctors then they would have been struck off for such behaviour but because they are not then the opportunities for the to behave in that way are unhindered and open to abuse and are regularly abused by those staff.
LikeLiked by 1 person
This is sadly true. The bullying, from PHSO staff must somehow be ingrained in their internal training program.
LikeLiked by 1 person
The whole investigation model with generic investigators and their use of clinical dvisers dealing with complaints is fatally flawed when looking at harmed patients. but sadly I am also learning many if not all of the same issues can occur with better trained investigators examining harm events with a system error agenda. More to follow in coming months. But how so many people have been won over by the PHSO, about to retire, totally escapes me. I saw him close and personal on 2 occasions. And his politicking and refusal to openly address well founded evidence was shocking if not unsurprising.
LikeLiked by 1 person
Great insights on the challenges faced by the Ombudsman in improving patient safety. It’s admirable how the team has worked towards professional development and transparency.
Thanks
LikeLike
Did you actually read the article?
LikeLiked by 2 people
Do you work for the PHSO because the comments in your post indicate that you do ?
LikeLike
I don’t.
LikeLike
Given you purport to not be an employee of the PHSO then are you, or the organisation you work, for used by the PHSO
LikeLike