Just as we come to the end of the 5-year strategy of restructuring under Dame Julie Mellor the new Ombudsman, Rob Behrens, announced this week the launch of a 3-year ‘back to basics’ strategy for the Parliamentary and Health Service Ombudsman (PHSO) Before we explore the new package of promises bear in mind that PHSO is 50 years old. Enough time for 16 previous 3-year strategies to iron out any wrinkles in procedures. Also, take into account that Rob Behrens has to pull off some kind of miracle to deliver any change given that PHSO will suffer a 24% cut in funding, they have lost 70 experienced staff in the move to Manchester and taken on at least 25 new (untrained) recruits to fill the gaps and to top it all they are presently working with a significant backlog of cases waiting for assessment, investigation and review. Against this backdrop, Mr Behrens is promising to make PHSO an ‘exemplary ombudsman service’. Will this new strategy help to ‘manage our expectations’ or promise more than it can deliver? PHSO Strategy 2018 -21
Our strategy 2018-21
Delivering an exemplary ombudsman service
We want to be an exemplary ombudsman service – one that continually learns from the best of what others are doing, while contributing to improvements elsewhere across the public sector and the wider ombudsman sector. We also want to continue building public confidence and trust in our service. While the PHSO Service Charter tells us that a significant majority of people who come to us say they get a good service, we know that too many think this is not the case and there is more we must do to address this.
Objective 1
To improve the quality of our service, while remaining independent, impartial and fair
We will introduce new ways of working that resolve cases more quickly, improving both the quality and timeliness of our decisions and the overall experience of people making complaints.
We will invest in our staff so they are equipped to deliver a professional casework service that remains sensitive to the complex, often tragic, issues that are brought to us.
Objective 2
To increase the transparency and impact of our casework
We will publish more information about our casework online to help improve public services, while enabling complainants, the public and organisations we investigate to have confidence in what we do.
We will target our insight reports so that important lessons from our casework and systemic reviews contribute to raising standards in public services.
Objective 3
To work in partnership to improve public services, especially frontline complaint handling
We will strengthen our relationships with other ombudsman services, and collaborate with others to improve how the public sector responds when things go wrong, from sharing good practice to offering training to complaint handlers.
Drawing insights from our casework, we will work with those best placed to apply the lessons learned to improve public services.
Well, he did say to HSJ that he wanted to ‘get back to basics’ and these three objectives (as in targets to achieve) represent nothing more than the core function of any Ombudsman service. Did the management at PHSO considered the outcomes of the previous strategy before they started ‘going backwards’? Here is a summary of the 2013/18 5-year strategy with the ambitious title of ‘More impact for more people’. our-strategic-plan-2013-2018-delivering-more-impact-more-people
So there we have it. PHSO has only just completed overhauling its investigation model, setting high standards and improving productivity. Working with stakeholders and parliament to ‘shine a light’ improve complaint handling and save money along the way. So confident were they back in 2013 they gave the following prediction of success. This must be a great starting place for Mr Behrens, lucky man.

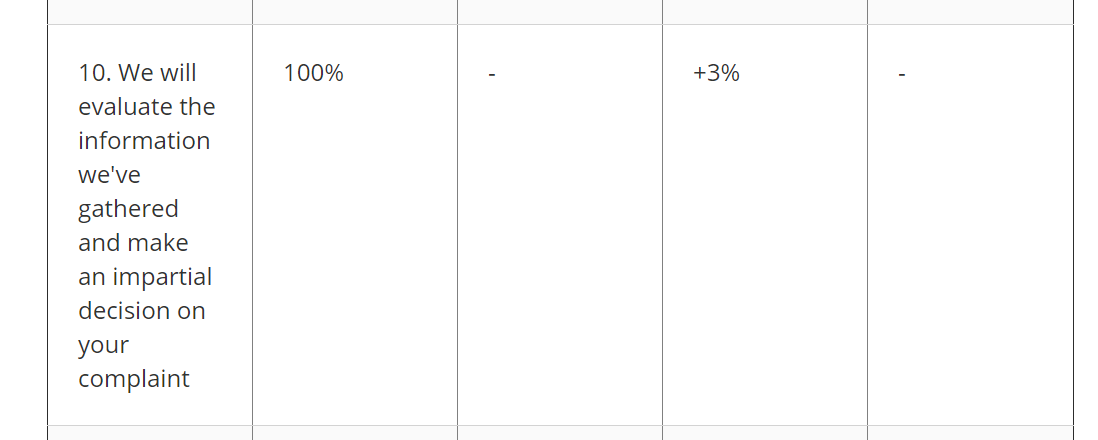
If more evidence of success were needed we can see from the much valued ‘Service Charter’ data that using these improved investigation models PHSO is able to make an impartial decision 100% of the time. Hard to improve on perfection so why does Mr Behrens feel the need to effectively negate the last five years of progress by restructuring the restructuring?
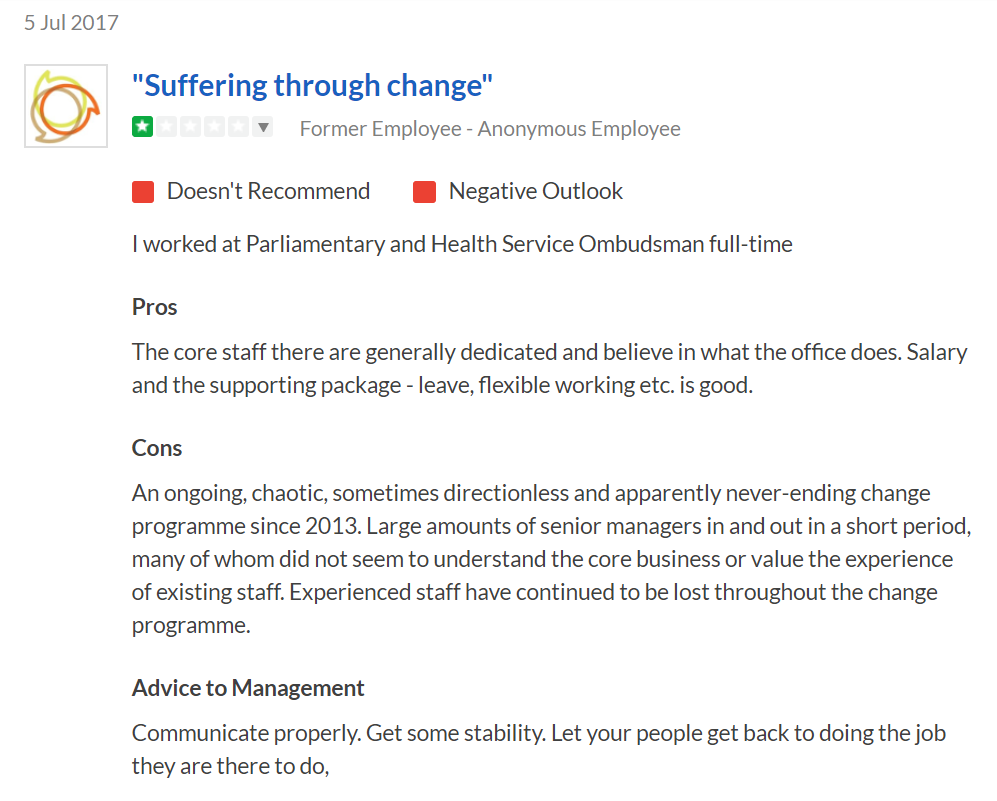
Certainly, some of the staff at PHSO feel that the continual imposition of new strategies is the very thing which prevents them getting on with their work.
 There are of course some advantages to having ‘a never-ending change programme’, it means that when criticism comes your way you can promise that improvement is just around the corner and ask for patience as you put in place the glowing rhetoric of your current plan. The jam tomorrow message has worn pretty thin with those of us who have been following the ups and downs, well mainly the downs of PHSO since 2012.
There are of course some advantages to having ‘a never-ending change programme’, it means that when criticism comes your way you can promise that improvement is just around the corner and ask for patience as you put in place the glowing rhetoric of your current plan. The jam tomorrow message has worn pretty thin with those of us who have been following the ups and downs, well mainly the downs of PHSO since 2012.
But perhaps we are being unfair to Rob Behrens. He has introduced some radical new ideas. If we can just wait until 2020/21 we can all benefit from the new ‘mediation’ service for early intervention and know that staff working on our complaints are fully ‘accredited’.
In 2020-21 we will:
- Begin accreditation of caseworkers.
- Evaluate mediation and other dispute resolution pilots, implementing the most successful as part of our new ‘Ombudsman toolbox’.
- Build the approach from our pilots into our training and accreditation programme, so staff are fully equipped to use these methods.
These new tools for the PHSO toolbox require pilot studies and new measures to be created to assess success. This could take a lot longer than 2021 to be up and running particularly as PHSO has still to find a body willing to provide the accreditation. Still fifty years of muddling through without the core functions in place (apparently) what harm in taking the time to get things right?
Dame Julie Mellor, despite her grand 5-year strategy, failed to deliver in all respects. She presided over a huge backlog in casework performance, a dramatic fall in employee satisfaction, financial scandals at PHSO and resigned early from her post having acted inappropriately when informed that her Deputy Ombudsman Mick Martin had been named in court proceedings and was found to have colluded with a colleague to cover up a valid complaint whilst working in the NHS. She simply lurched from one crisis to another. how-do-you-solve-a-problem-like-dame-mellor
Consequently, both the Ombudsman and Deputy Ombudsman left the service before seeing the fruits of their labour. But what exactly was the legacy left for Rob Behrens to inherit at the end of her five-year change programme? A look at the last published Board Minutes for PHSO gives us some idea of what is going on behind the scenes and it doesn’t look good.
From September 2017 (latest published) we can see the following issues:
PHSO_Board_Minutes_28_September_2017
On the staffing issue, Amanda Campbell CEO confirmed the loss of 70 staff fro,m the London office.
9.6 Amanda Campbell acknowledged that staff had felt let down by the slow pace
of consultation and change. However some difficult decisions had been
made and only eight compulsory redundancies had been necessary, from a
reduction in staffing of over 70 posts.
Having survived the ‘cull’ there are issues with staff engagement.
9.10 The Board discussed the contents of the report. Ruth Sawtell said that it had
been disappointing to see the fall in staff engagement reported in the June 2017 pulse survey.
Amanda Campbell said that the survey had been taken in the middle of the collective consultation period at a time of maximum uncertainty. However a significant change was not expected in the October 2017 survey, as transition was still underway.
Always look on the bright side Amanda but you need to take the staff with you when sharing your vision of an exemplary Ombudsman service.
9.3 Amanda Campbell advised that there were now many changes happening
simultaneously and quickly. She said she wished to assure the Board that PHSO recognised and were managing the volume of activity across the organisation.
9.8 Amanda Campbell recognised that communications with staff about the change programme had been poor. As a result of this a weekly cascade was now in place that had received positive feedback from staff.
Oh dear, not managing change well was the same complaint from staff under the previous Ombudsman. Referring to the ‘training programme’ which is essentially the key to all the improvements put forward by Rob Behrens there was this comment.
9.12 Jon Shortridge commended the training programme but said that it must go beyond a ‘sheep dip’ approach. Amanda Campbell reported that, following the training, experienced staff should continue to support new staff. Staff were integral to the design and delivery of training, which was modular and was aimed at meeting the range of different needs. The training would eventually lead to accreditation.
No mention here that PHSO had just lost 70 experienced staff and taken on at least 25 new recruits in Manchester as their replacement. So the experienced staff must meet their targets to get the backlog down whilst supporting new arrivals who had received their ‘sheep dip’ training. However, it was recognised by Ms Campbell that the training of new recruits and the re-training of all current staff would have an impact on the backlog.
11.4 Unallocated assessments and investigations had both risen significantly since the end of Q1 and were likely to increase further as caseworkers were taken offline for training. Amanda Campbell tabled a chart showing projections that by the end of the business year there would be 788 unallocated assessments and 567 unallocated investigations. (A copy of the table is attached to these minutes at Appendix 2). The numbers would then reduce gradually, with assessments projected to be at or close to zero by August 2018, and investigations to be at or close to zero by December 2018. These projections were based on a mitigation agreed by the Executive Board on 27 September 2017, to recruit 25 caseworkers above establishment.
One minute it all relies on staff who are professional to accredited standards and the next it is deemed by the Board perfectly acceptable to take 25 people with no experience and with minimum training and have them manage complex cases where the complainant has already had a significant wait. Perhaps the following statement reveals how PHSO management ensure that staff (new and old) caught in the trauma of reallocation and restructure perform to a given target.
9.13 Julia Tabreham expressed concern about the reported rise in bullying in the pulse survey. Amanda Campbell replied that there was no increase in staff saying that they had personally experienced bullying. Rather there was a perception of bullying through performance targets and the way the consultation had been managed. The trade union side had been asked to provide evidence of incidents of bullying, but no direct evidence had been received. There was perhaps a need to be more clear about what was meant by bullying and harassment.
Ahh, just a ‘perception’ of bullying and staff not realising what ‘bullying and harassment’ really is. Well if you feel bullied I guess you would call it bullying but management know best and seem to have the only dictionary of terminology that matters. The title of their policy on casework does suggest rather a heavy hand.
11.2 Amanda Campbell tabled before the Board an extract from a presentation first made by Rebecca Marsh to the Quality Committee on 14 September 2017, on ‘Driving the Quality of Casework at PHSO’. (The presentation is attached to these minutes at Appendix 1). The presentation set out a list of areas where it was perceived that there were quality issues, and identified actions planned for dealing with three of these areas: Thoroughness,
Communications and Clinical Advice. Elisabeth Davies said that this paper had been discussed by the Quality Committee, who had focussed on the potential quality impacts of the Target Operating Model.
‘Driving the Quality of Casework’ does sound pretty hostile, particularly when you bear in mind that there is a major problem at PHSO with the technology available to do the job.
13.14 ICT was now a RED risk. A number of issues had arisen which had the potential to impact on service delivery in future. Mitigations had been agreed and were outlined in the risk register. It was recognised that PHSO now needed to carry out a full review of the ICT structure, looking at the robustness of service provision and how the systems delivered the Corporate Strategy.
Poor things, they have yet to receive all the new training and wisdom brought to PHSO by a real Ombudsman, Prof Behrens CBE but already they are being ‘driven’ to perform without the IT systems to support their work. And what of Mr Behrens the real Ombudsman, how did he share his vision with the Executive Board in order to lead the way to an exemplary service. Only one statement in the entire meeting was assigned to the man himself and you can see it below.
10.5 Rob Behrens highlighted his series of engagement meetings with staff. These had been very productive and the output from the meetings would be fed into the strategic plan for 2018-21.
Now that sounds familiar. Mr Behrens regularly has ‘productive meetings’ even if no-one else agrees with him. Can’t possibly be his fault then that the sickness levels at PHSO have gone through the roof.
13.2 The Board were concerned that PHSO were very close to the sickness absence
target. Gill Kilpatrick said that PHSO were looking at this very closely to understand the trend.
Mmm, Board has no idea why staff are going off sick. Could it possibly be linked to rapid and repeated change, loss of experienced staff, lack of essential IT resources and a hostile working environment? They will have to ponder on that one.
Given this is the current state of affairs at PHSO it is difficult to have any confidence that the new 3-year strategy will be any more successful than the previous 5-year strategy. But the real benefit of a change programme is that it helps to boost public confidence and stops critics in their tracks by saying ‘we are doing something’.
PHSO – a continual journey towards excellence
which never arrives.


Contributor 7 the kind of problems you address have been going on for years, with hypocrisy amongst politicians who oversee the PHSO and LGO at its highest level ever.
I wonder how many relatives of the 450 deceased recently reported in Kent were given the “bums rush” / Brush off by PHSO.
LikeLiked by 1 person
Back to Basics? There appears to be less effort on investigating, revealing failures and improving the PHSO service for learning or rectification for the complainant, and much more emphasis on PR, spin and adjustment (censorship) of what is published.
Things like ‘what cases can we publish to claim ‘success”, ‘how do we look’; how do we present ourselves’; ‘how can we tart-up our image’ etc. etc. but still failing in attitude, purpose, service standard, or credible response: an overall incompetence in running a business that is supposed to be accountable to its ‘share holders’ i.e. the public, but in reality is accountable to nobody in the sense of service quality or value.
Look closely at the PHSO “success stories” to see what pressure had to be applied for any steps to be taken at all. For every published story there could be published 100 serious failures brushed under the carpet; and that is what we are seeing now on social media – the failure of an already unfit 20th Cen. carry-over process grappling with an educated 21st Cen. public who are tired of lies, cover-up, and piecemeal “settlements” which totally deny the point of the complaint.
The cost of this to UK.org is rising negligence and claims, avoidable harm and deaths, and the cost to NHS.org in misdirected effort hanging-on to unsuitable workers out of touch with modern practices, and long past their best-by date.
This is not said with disrespect for the many NHS workers going above and beyond their duty to make a difference (the responsible workers; the whistle-blowers?) who do their best to Care. Make no mistake I commend them and I have witnessed all sorts in action; but it depresses me that 21st Cen has brought few useful changes in healthcare and has revealed its worst side to me.
Of all the worries a parent might have about their children and what risks the future may hold I did not expect one of mine to succumb to NHS negligence, and then (as an explanation; an excuse?) for me be told “he was non-compliant”; and “he would probably have died anyway” by this disgusting and abusive Office – the PHSO.
And now it wants to turn the clock back. Could that mean from 20th to 19th Cen?
People are dying unnecessarily whilst the PHSO leadership fails and falters.
LikeLike
You have hit the nail firmly on the head here. We can all see through the PR spin but still they persist in the charade that with a bit of tweaking all will soon be well at PHSO.
LikeLiked by 1 person
lots of evidence, undisputed by the PHSO that reforms, back to basics, basic ombudsmanship are not fit for purpose and lip service to the years and reams of complainant feedback how they have failed-for someone whose multitude of complaints was upheld but it had no visible impact and met RB , it is back to the future-lip service- a waste of money
http://phsothefacts.com/a-meeting-with-mr-behrens-learning-or-lip-service/
LikeLike
“We will publish more information about our casework online to help improve public services”
Well if they are like the LGO (their bosom buddy) then they will be publishing altered versions of the facts online that nobody can reply to, to say it’s wrong. They alter the basis of the investigation so that it bears little resemblance to the complaint that was made and they can put up anything they choose online. Then send out marketing customers with questions about politeness and efficiency whilst avoiding the actual problems of ignoring evidence, rebundling the complaint into another entity, refusing to investigate a valid complaint or focusing on trivial aspects.
“Dame Julie Mellor, despite her grand 5-year strategy, failed to deliver in all respects.”
And yet she left with a pat on the back, a gold star and through that revolving door.
As for the accreditation…really..? I mean, there was me thinking all that was needed to be a good caseworker was some understanding of the issue you were looking at, some honesty and good old common sense. But that would clearly be asking too much, Behrens wouldn’t want to increase the uphold rate now would he…
Does the PHSO Board include anyone from PACAC or do they have to be separate? All I can say is, if the board is anything like PACAC, they simply turn a blind eye.
It’s vile and disgusting what public money is being spent on. The grief, distress and trauma people are suffering having got as far as PHSO only to be kicked in the teeth. Irrational, unjust and devastating decisions, which if you disagree with, you are labelled vexatious and put in the post-review pot to be ignored.
LikeLiked by 1 person
The level of information provided by PHSO is vague to say the least.
The level of competence is appalling.
I received a copy of the response from the NHS Trust I complained about three months after the decision was made by the ombudsman.
I complained about it to the PHSO and received a letter of apology without any further comments other than a letter from a Director telling me they would not take the matter any further. Also that any further correspondence would be noted, filed and shredded 12 months later .
The arrogance is appalling and would not be accepted anywhere else on the planet
LikeLiked by 1 person
Interesting to note today that Jeremy Hunt has admitted there was a computer error in NHS England system relating to Cancer and that over 450,000 people were not contacted for further tests. It was also probable that up to 230 people had died as a result. Also notable that Bernard Jenkins M.P. is still bashing on about Brexit when he should be looking at PHSO and its long term negligence. Politicians who tell the truth and own up to problems are a very rare breed.
.
LikeLiked by 1 person
Having received many unintelligible and frankly offensive replies from the PHSO over the years Behrens is going to have to do something about the deaf ears at PHSO where your experiences in trauma are ‘opinions’ and practitioner’s and advisers (who were never there) ‘opinions’ become dominating facts in putting down the complainant. This is into serious breach of .disability law – and FOIs confirmed they had no policy in assessing complainants standpoint. Accreditation in any skill will be extremely unlikely. Identifying negligence now appears to be all in question too. Basically no change here.
LikeLiked by 1 person
The cover ups by politicians of all parties is comparable to the Windrush scandal which has led to the resignation of the Home Secretary this morning . When will Bernard Jenkins resign.
LikeLiked by 1 person
‘The Board’ are responsible for the PHSO and appear over time to be unable to make any positive progress in raising the quality of the admitted ‘poor service’.
For years now people have been let down and so no lessons have been learnt by failing authorities.
Time to take a look at the performance of those responsible. Those who say they don’t look at individual cases, but how can they be sure of what’s going on if they don’t look at individual cases?
Are they infringing our human rights? Or other laws?
Time to shift the forces on to those with the responsibility for seeing that the ‘Last Bastion of Justice ‘ does just that. Administers Justice.
The shape-shifting must stop. People with long-standing grievances need to see the justice they would have received but for the ‘poor service’ of PHSO and the Board are responsible!
LikeLiked by 1 person
Anne B. PHSO are very bad at data protection. I was promised before the final report on my complaint in March 2016 that I would receive redacted copies of the evidence from the NHS trust.. I received un redacted copies of the evidence four months after the final report . I have had an apology but nothing else since.
Apologies come cheap.
As has been proven this week by the way Windrush immigrants have been treated by both civil servant and Home office ministers
LikeLiked by 1 person
I suspected that they were, so I think I’ll see how much paperwork I can cause them. Who knows, it might just motivate them, and if it doesn’t, there’s a certain sneaky pleasure in presenting them with a service failure and a data protection act breach that they have to record. I then do a FOI to show how many of them there have been and submit it to PACAC as my equivalent of a Christmas card. Last year they quoted one of my statistics and the PHSO and Chief Exec claimed it wasn’t right and had to clarify it. Which was fun, because I think it’s good for them to squirm. They need the exercise!
LikeLike
We need desk paperweights saying “the Buck Stops Here”!!
LikeLiked by 1 person
Most PHSO reports on the failings of the NHS at all levels are accurate. Problem is nobody does anything to improve the problem and to most people ( victims of the system) the frustration of doing nothing is very distressing .
LikeLiked by 1 person
Must deal with corruption from the past before he can move on. Cant just leave a trail of broken minds, bones and ashes of the kids he let down.
LikeLiked by 1 person
An accurate summing up to date highlighting lots of jam still to come for lots of tomorrows, the only conclusion available after responding to the PHSO’s publicised agenda on how complaints are handled. The new ombudsman though is perfection as the new strategy really ensures that those complained about continue to enjoy complete protection accountability and tranparency (popular words, much used for the PHSO’s previous promises), whilst those invited to complain provide valuable casework studies, with this information shared ‘about what went wrong, so mistakes can be avoided in future’ (although it is not clear who learns what) with the new complainants discovering the ever-decreasing circles of nowhereland to add insult and further distress to injury.
But it reads convincingly and beckons…
LikeLike
When the ombudsman released their new strategy.they sent a group email to everyone who’d responded to their consultation letting them know it had been posted but they didn’t blind copy it so we all received details of everyone’s email address. I pointed this out to them and they recalled it 4 hours later, apologised and assured us that procedures would be altered so it wouldn’t happen again.
I’ve asked for an explanation as to why this is the second time in 6 months that they’ve breached the Data Protection Act with my private data. If no answer by Friday I’ll contact the ICO and report my concerns.
In the meantime, I have a screen shot of the original message and it’s interesting to see that most of the stakeholders are from NHS organisations and the PHSO staff member referred to us as ‘colleagues’ in her email. Presumably this is another example of their approach to neutrality?
LikeLiked by 1 person
When my comments to the House of Commons PACAC were published on July 16th. 2016 on line they were not redacted until three days later.
As far as I know the people named by me have not yet objected to their names being publishes for the whole world to see.
LikeLiked by 1 person
Mr. Behrens need not worry about publicity for his organisation. The first thing any body within the NHS ( ( G.P. Or NHS Trust) does, when first receiving a written complaint, points out that if you are not satisfied with their investigation and reply you can take your complaint to the P.H.S.O. They are all well aware just how hopeless the PHSO really are , so pass the buck with considerable confidence , in the knowledge that little or nothing will happen. I am confident that most people on this site have had that experience.
LikeLike
Just gone past the royal courts of justice and see ipso is in court re free press, there’s some kind of demo going on…
LikeLike
I think I’ve worked out the corporate strategy. It’s ‘let’s all stick our fingers in our ears, cover our eyes and sing ‘lalala everything wil soon be wonderful.’
LikeLike
That’s about right Ann.
LikeLike